Blog
- Transcranial Magnetic Stimulation: A Treatment for Depression
- By Jason von Stietz
- February 27, 2015
-

Photo Credit: APA Monitor Transcranial magnetic stimulations (TMS) is becoming more commonly utilized as a treatment of medication resistant depressive symptoms. TMS is a treatment in which the left frontal cortex, which is often underactivated in depressed individuals, is stimulated in attempt to regulate the neuronal circuits involved in mood. This treatment can take 20 to 30 sessions and lead to significant improvements in mood. TMS was discussed in a recent article in APA Monitor:
Sharon Gray* has had depression for most of her life. She was first diagnosed at 30, but she believes her depression started much earlier. Now 61, the retired police lieutenant from Columbus, Ohio, has seen clinical psychologists and psychiatrists and taken antidepressant medication for most of the last three decades. The treatments have left her functional, she says, but still mildly depressed. Every so often, she's suffered periods of more severe depression.
In 2007, desperate for a new option, she flew to Atlanta for a therapy that, at the time, was still experimental: transcranial magnetic stimulation, or TMS. Just past the halfway point in the monthlong course of treatment, "I had what I thought were miraculous improvements," Gray says. "I went to sleep on a Tuesday night depressed, and woke up Wednesday morning not depressed."
To celebrate, she went jewelry shopping. If that sounds trivial, think again: "I had not been interested in my appearance for so long," she says.
The following year, in 2008, the Food and Drug Administration (FDA) approved TMS as a treatment for people with major depression who have failed to respond to at least one antidepressant. Initially, the agency approved just one TMS device, called NeuroStar, made by the company Neuronetics. In 2013, the FDA approved a second device, manufactured by Brainsway.
In the years since FDA sanctioned the therapy, TMS treatment centers have been popping up across the country. Slowly, insurance companies have begun to cover the non-invasive, though costly, treatments. But plenty of questions about TMS still linger, including how best to deliver it, which patients make the best candidates and even what, exactly, the device is doing in the brain.
Despite that, the therapy is gaining support from patients and mental health providers alike. "I think it's a promising treatment," says William McDonald, MD, a psychiatrist at Emory University School of Medicine who was involved in the clinical trials that led to the approval of the NeuroStar device. "I'm a skeptic. But if I had significant depression and I had failed one or two antidepressants, I'd have to consider TMS."
Changing neural networks
TMS is typically administered by a physician or a nurse. The procedure involves a non-invasive machine placed against the scalp. The device sends short but intense magnetic pulses into the brain, where they generate an electric current. The pulses are centered over the left prefrontal cortex, an area that often shows abnormal electrical activity in depressed patients. A typical course of TMS therapy involves 20 to 30 sessions, generally given in three to five treatments per week for four to six weeks. The full course of therapy with the pricey machines can cost $6,000 to $12,000. During the treatments, patients remain awake and alert, seated in a chair while a physician or a nurse places the device against the scalp.
TMS has become a promising treatment alternative for the estimated 30 percent to 50 percent of people with depression who don't respond sufficiently to antidepressant medications. One option commonly offered to such patients is electroconvulsive therapy (ECT), a procedure in which electrical currents are sent through the brain to trigger a short seizure. ECT has been available in the United States for more than 70 years. Administered several times per week over three to four weeks, ECT can be effective at alleviating major depressive disorder.
However, ECT has some significant drawbacks. It can cause confusion and memory loss. Plus, it must be administered under anesthesia, which comes with risks of its own and adds preparation and recovery time to each session.
Gray had tried ECT, but her doctor discontinued the treatment after she experienced serious memory loss. "I have no recollection of that entire two-plus weeks," she says. "I live alone, and it was scary."
TMS, by contrast, is administered while patients are awake. "You sit in a chair, it takes about 30 minutes, and then you can get up and drive yourself home," says McDonald. Side effects are minimal; headache and muscle soreness are the most common complaints. Though there is a small risk of seizure, it's reportedly comparable to the seizure risk associated with antidepressant medications. Compared to ECT, Gray says, "TMS is a walk in the park."
But like antidepressant medication and ECT, it's not entirely clear how TMS is acting on the brain. "The theory is that when this stimulation occurs in the left frontal brain, it spreads to the underlying deeper areas of the brain that are involved in regulation of mood. When we do it over and over again, it normalizes the neuronal circuits involved in depression," says Ananda Pandurangi, MD, a psychiatrist at the Virginia Commonwealth University School of Medicine.
Like ECT, TMS appears to reset the system. But instead of jump-starting the entire brain, as ECT does, the magnetic therapy is much more targeted, says Megan Schabbing, MD, a psychiatrist at OhioHealth Riverside Methodist Hospital who treated Gray with TMS. "That's undoubtedly why it's so well tolerated," she says, "but this treatment provides a novel approach to the transformation of neural networks."
Real-world results
Mark George, MD, a neurologist/psychiatrist at the Medical University of South Carolina and editor of the journal Brain Stimulation, has been exploring the use of TMS for depression since the early 1990s. At that time, he says, most neurologists believed brain stimulation was only successful if it induced a seizure, as in ECT.
But George believed that the gentler electric currents generated by TMS could also be effective if they were delivered repeatedly. Small changes add up, he says. Repeated exercise can strengthen a weak muscle. And in depression, psychotherapy can be an effective treatment over time. "You can exercise brain circuits by retraining how you think," George says. "We know repeated minor changes to the system can get the system better."
George was the co-chair of a multisite, randomized clinical trial of TMS sponsored by the National Institute of Mental Health. The study enrolled patients with treatment-resistant major depressive disorder between 2004 and 2009. After three weeks of either active TMS or a sham treatment, all patients were offered an additional three weeks of guaranteed TMS. Those who received TMS were four times as likely to achieve remission as compared with patients who received a sham treatment, the researchers found (Archives of General Psychiatry, 2010). The results were fairly modest, however — about a 30 percent remission rate for TMS at the end of the full six weeks, compared with perhaps 60 percent for ECT, George says.
Yet it now seems that TMS may be more effective than the initial trials suggested. Linda Carpenter, MD, a psychiatrist at Brown University School of Medicine, and colleagues studied TMS as it's used in the real world. Across 42 TMS clinics in the United States, they found that 58 percent of patients showed improvement, including 37 percent who achieved full remission (Depression and Anxiety, 2012).
Anecdotally, many practitioners appear to be pleasantly surprised by the treatment's success. While the NIH-sponsored trial found about two in 10 patients experienced remission following TMS, George, Pandurangi, and Schabbing all say they've seen higher remission rates among the patients they've treated. "It has really exceeded my expectations," Schabbing says.
The strict protocols in the clinical trials probably account for some of the difference. Trial participants were required to stop taking medications during the course of TMS treatment. They could continue their psychotherapy, but they couldn't increase the frequency of their sessions.
Patients receiving TMS in the real world have many more options, says Pandurangi. They can continue taking medications to which they may have had a partial response, and they can see therapists whenever they'd like. Those options appear to improve patient outcomes. "We mix and match anything and everything we have to make the patient feel better," he says.
Everything's a question
While TMS shows promise, it's certainly no miracle cure. Some of the patients who responded positively to TMS have experienced remissions lasting months or even years, but follow-up booster sessions every few weeks or months may help prevent a relapse.
About six months after her incredible improvement in 2007, Gray says, her depression began to resurface. She underwent a second course, this time at a clinic in Vancouver, Canada. While she felt better, her improvement was more modest the second time around.
Gray had paid out of pocket for the pricey therapy and was quickly burning through her retirement savings. She couldn't afford another round, even after her depression resurfaced months later. "So I puttered along until a few years ago, when I had another deep depression," she says.
By then the treatment had been approved by the FDA. Still, it took Gray multiple applications over several years before her insurance company agreed to cover the treatment. She finally underwent a third course of TMS in 2014. "I feel pretty good," she says. "I've had two pretty bad pieces of news in the last couple weeks and I didn't crumble."
Now Gray is planning to have a maintenance course of TMS every month or so, in hopes that it will keep her depression at bay. She's still not sure if her insurance will pay for those booster sessions — and that's not the only thing that remains unclear about maintenance TMS.
French researchers recently reported that patients who received maintenance TMS were significantly less likely to relapse than those who did not receive boosters (Journal of Affective Disorders, 2013). But the study was small, and the best way to administer such treatments is far from settled. "The protocols for maintenance boosters don't exist. Nothing has been approved by the FDA, so we devise our own protocols," Pandurangi says.
In fact, he adds, when it comes to TMS, "almost everything is a question." What's the best frequency and intensity of the magnetic pulse? How many total treatments should patients receive, over how many days or weeks? Where on the scalp should the current be directed?
Researchers are a long way from fine-tuning the technique, George agrees. "All the things we did in the first studies used a good first approximation, and it turned out that it worked," he says. "However, it would be inconceivable that the first approximations were also the best approximations."
There's some evidence the total amount of brain stimulation is what matters, rather than the number of calendar days spent in treatment, George says. In a recent pilot study, George and his colleagues tested TMS as a treatment for patients hospitalized during a suicidal crisis. Patients received nine TMS treatments in just three days. They experienced no serious side effects from the rapid-fire course of treatment, George says, and those who received TMS showed more improvements on the first day than did control subjects who received a sham treatment (Brain Stimulation, 2014).
"They got unsuicidal very quickly," George says — though he acknowledges that more research and larger samples are required to fully test the approach.
While many questions remain, scientists who study the device say it's a valuable tool for psychologists to keep in mind when referring patients with difficult-to-treat depression. "Psychologists should know it's a good treatment option for patients who have failed to respond to or tolerate antidepressant medication," Schabbing says.
Fire together, wire together
As magnetic brain stimulation continues to be tested in the real world, researchers are considering whether to expand its use. Psychotherapy and antidepressants are highly effective treatments for many people with depression. They're also more convenient and less expensive, so TMS is unlikely to become a first-line therapy for depression that responds to other treatment. But it has potential for treating other conditions.
Researchers have found that TMS could be effective in treating vascular depression following stroke, for example (Archives of General Psychiatry, 2008). Others are studying TMS as a possible treatment for disorders including schizophrenia, attention deficit-hyperactivity disorder and post-traumatic stress disorder. "Following the success with depression, almost everybody who treats brain diseases is thinking about whether you could use TMS," George says.
So far, however, the results are mixed. "The one exception is in the treatment of pain," George says. Data suggests TMS could be helpful in treating both acute pain and chronic pain conditions such as fibromyalgia — but to date, no companies have sought FDA approval for that use, he adds.
Meanwhile, scientists are also exploring how to engage patients in order to maximize the effectiveness of TMS during treatment for depression. "There's a concept that says ‘neurons that fire together wire together,'" says George. According to this theory, brain cells might be more receptive to treatments when they're actively engaged in some task.
For instance, preliminary research suggests patients might experience greater improvements if they receive TMS while simultaneously undergoing cognitive-behavioral therapy, George says. If this line of research pans out, psychologists could play an important role by providing psychosocial therapy while patients are in the TMS chair.
And TMS may be just the beginning. Scientists are exploring other methods of stimulating the brain, including pulsed ultrasound and optogenetic stimulation. The research could open up important new avenues for treating mood disorders and mental illness, Pandurangi says. "It's exciting to see what's coming next."
Kirsten Weir is a journalist in Minneapolis.
*Not her real name.
Read the original article Here
- Comments (0)
- How the Right Hemisphere Might Assist the Left Following a Stroke
- By Jason von Stietz
- February 25, 2015
-
Photo Credit: Wellcome Images Can the brain reorganize itself following brain damage? Researchers at George Washington University investigated how the right hemisphere might assist the left hemisphere following damage caused by a stroke. Findings indicated that the right hemisphere is able to represent both left and right visual fields in a sample of healthy adults. This finding could have interesting implications for victims of strokes. NeuroScientistNews discussed the study in a recent article:
A new study conducted by a researcher at the George Washington University suggests that the right hemisphere of the brain may be able to assist a damaged left hemisphere in protecting visual attention after a stroke.
Summer Sheremata, a postdoctoral research fellow in the Attention and Cognition Laboratory in the Columbian College of Arts and Sciences, led the study. The paper, "Hemisphere-Dependent Attentional Modulation of Human Parietal Visual Field Representations," was published in the Journal of Neuroscience.
"Patients with damage to the right hemisphere often fail to visually perceive objects on their left, but the reverse is much less common. That is, damage to the left hemisphere does not typically lead to deficits in attention," Dr. Sheremata said. "Psychologists have hypothesized that the right hemisphere could help out the left hemisphere in attending to objects on the right, both in healthy individuals and patients recovering from stroke, but until now it remained an assumption."
The research was conducted at the University of California, Berkeley, with senior author Michael Silver, associate professor of optometry and vision science and neuroscience. Participants' brain activity was measured using fMRI while they used their attention in two different ways:
♦ Paying attention to a central box, ignoring a moving object in the background, and
♦ Ignoring the central box and paying attention to the moving object in the background.The first scenario measures the visual response, confirming that the right side of the brain represents the left visual field and that the left side of the brain represents the right visual field. The second scenario tests the effects of visual attention and indicates that while the left side of the brain only focused on the right visual field, the right side of the brain was able to represent both sides of the visual field. Visual field representations are included in a figure in the study.
While the research was conducted on healthy, non-stroke patients, the results suggest a possible brain mechanism for how the visual field can be recovered if it is damaged by a stroke.
"The results demonstrate that the tasks we do every day change how the brain pays attention to the world around us. By understanding how these changes occur in healthy individuals, we can focus on behaviors that are impaired in stroke patients and provide a focus for rehabilitation," Dr. Sheremata said.
To further the research, Dr. Sheremata plans to study how these effects influence behavior in stroke patients and healthy individuals during attention and memory. Her next round of studies is being conducted at the George Washington University.
Read the original article Here
- Comments (0)
- How the Teenage Brain Responds in Social Situations
- By Jason von Stietz
- February 11, 2015
-
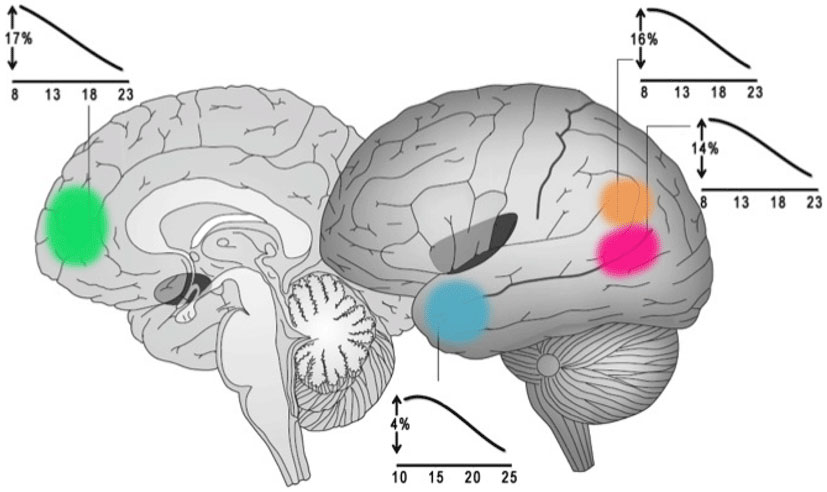
Photo Credit: Scientific American How does the teenage brain react when seeing a friend? How about a stranger? What happens to the brain when viewing Facebook? Researchers have studied how the brain responds in social situation, in daily life and online. Amanda Baker discusses the responses of the teenage brain in a recent article in Scientific American:
While we all may vary on just how much time we like spending with other people, humans are overall very social beings. Scientists have already found this to be reflected in our health and well-being – with social isolation being associated with more depression, worse health, and a shorter life. Looking even deeper, they find evidence of our social nature reflected in the very structure of our brains.
Just thinking through your daily interactions with your friends or siblings probably gives you dozens of examples of times when it was important to interpret or predict the feelings and behaviors of other people. Our brains agree. Over time parts of our brains have been developed specifically for those tasks, but apparently not all social interaction was created equally.
When researchers study the brains of people trying to predict the thoughts and feelings of others, they can actually see a difference in the brain activity depending on whether that person is trying to understand a friend versus a stranger. Even at the level of blood flowing through your brain, you treat people you know well differently than people you don’t.
These social interactions also extend into another important area of the brain: the nucleus accumbens. This structure is key in the reward system of the brain, with activity being associated with things that leave you feeling good. Curious if this could have a direct connection with behavior, one group of scientists studied a very current part of our behavior as modern social beings: Facebook use.
The researchers had a group participants record short videos about themselves. The participants believed that these videos would be viewed by anonymous reviewers who would then pick 10-15 adjectives describing their perception of the participant. The next day, participants were placed in an MRI and the nucleus accumbens was monitored while they heard two sets of adjectives: those selected by reviewers to describe the participant and those selected to describe one of the other participants.
In reality, the adjectives had been pre-selected by the researchers, allowing them measure activity in the nucleus accumbens when the participant heard that the reviewers thought highly of them and compare it to activity while they heard that the reviewers thought highly of the other participant.
The researchers found that the participants whose brains gave a bigger reward for their own feedback compared to the feedback of others were more likely to use Facebook more intensely. Considering that Facebook allows for personal feedback in the form of likes and comments, as well as the ability to monitor the success and approval of others, this correlation seems to make sense.
Differences in these parts of the brain can account for some variability between individuals, but what about differences that seem to be defined by age?
Many areas of the brain grow and develop as you age, and the areas responsible for social emotions are no different. Between the ages of four and five, you start to develop the ability to understand that people around you could be having thoughts or emotions that are different than your own. Further important changes occur during a period that society often seems to single out as the pinnacle for being different: adolescence.
Adolescence – the period extending from puberty to the point of independent stability – is often portrayed as a very dramatic time with a new emphasis placed on the importance of friendships and social input. Researchers have even found during this period that many adolescents value the input of their peers even over the input of their family.
The current generation of teens are faced with the addition of social media and digital content to their lives, additions which seem to have pushed many age-driven differences in behavior into a new arena. There are even notable differences in the way the current generation of teens consumes media. While older adults watch ~47 hours per week of television on average, current teens are only watching about 19 hours. Instead, they are consuming vast amounts of online video – like Youtube, Vine, and vlogs.
In traditional television or movies the stars and the plots are often mysterious people and ideas that cannot be touched by the outside world. In contrast, young vloggers and stars of Youtube and Vine often host Q&A sessions with their fans; integrate feedback into future content; and express their gratitude not to their fans, but to their “6 million friends.”
Move up just a few years to young adults and there is already a shift, with this group watching five times as much television as online video. At least some part of that difference can perhaps be accounted for with changes that occur in this period to the brain itself.
One of the areas going through important structural changes in this period – with additions of gray matter and changes in shape – is the area that deals with “social emotions.” Social emotions are those that require you to consider what others might be thinking – like guilt or embarrassment – rather than your own emotional experience – like fear. When researchers ask adolescents and adults to explain certain emotions, both groups feel and describe them in the same way. But the activity that is happening in the brain, and the way that information is being processed, differs between the two groups.
Another group of researchers wanted to understand how these differences in brain processing might eventually translate in to feelings or behavior. They set up a virtual game in which participants got to play catch with two other onscreen characters. At some point during the game the other two characters begin just to throw to each other, excluding the participant from the game. The adolescents reported more anxiety and negative feelings at being excluded than the older participants.
Because some of the brain areas still growing during adolescence include those involved with social emotions, researchers would like to know if this could lead to additional importance being assigned to those signals – the approval and disapproval of your peers – than later in life. These researchers highlight the role that this could be playing in decision-making processes. Consider that two people could see the same risks and rewards in a decision – such as smoking a cigarette. By changing the value assigned to one of these factors, such as the social outcomes, one could tip the decision in one direction or the other. If the development of the social-emotion processing in the brain causes more attention or importance to be assigned to those emotions during that period, the social outcomes could seem more extreme in their potential risk or reward in the adolescent brain.
As we learn more about the way our brains process social information and emotions, we can better understand the differences between individuals and between age groups. But as technology continues to develop, providing new social arenas and sources of feedback and comparison, we are faced with new expressions of these differences in behavior. With six billion hours of Youtube being consumed every month, it is not just scientists who are trying to understand these behaviors, but advertisers and media companies. It will be exciting to see how things change as the current generation of teens grows up.
Read the original article Here
- Comments (0)
- Brain Studies Suggest Ways to Improve Learning
- By Jason von Stietz
- February 6, 2015
-

Photo Credit: Scientific American Do brain training games work? Neuroscientists often study the underlying processes involved in learning in hopes of developing interventions to help children with learning difficulties, as well as to booster learning in other children. However, parent’s and educators are often unsure of what interventions to use, as evidence of their effectiveness are often mixed. Gary Stix discussed studies examining learning processes and interventions in a recent article of Scientific American:
Eight-month-old Lucas Kronmiller has just had the surface of his largely hairless head fitted with a cap of 128 electrodes. A research assistant in front of him is frantically blowing bubbles to entertain him. But Lucas seems calm and content. He has, after all, come here, to the Infancy Studies Laboratory at Rutgers University, repeatedly since he was just four months old, so today is nothing unusual. He—like more than 1,000 other youngsters over the past 15 years—is helping April A. Benasich and her colleagues to find out whether, even at the earliest age, it is possible to ascertain if a child will go on to experience difficulties in language that will prove a burdensome handicap when first entering elementary school.
Benasich is one of a cadre of researchers who have been employing brain-recording techniques to understand the essential processes that underlie learning. The new science of neuroeducation seeks the answers to questions that have always perplexed cognitive psychologists and pedagogues.
How, for instance, does a newborn's ability to process sounds and images relate to the child's capacity to learn letters and words a few years later? What does a youngster's ability for staying mentally focused in preschool mean for later academic success? What can educators do to foster children's social skills—also vital in the classroom? Such studies can complement the wealth of knowledge established by psychological and educational research programs.
They also promise to offer new ideas, grounded in brain science, for making better learners and for preparing babies and toddlers for reading, writing, arithmetic, and survival in the complex social network of nursery school and beyond. Much of this work focuses on the first years of life and the early grades of elementary school because some studies show that the brain is most able to change at that time.
The Aha! Instant
Benasich studies anomalies in the way the brains of the youngest children perceive sound, a cognitive process fundamental to language understanding, which, in turn, forms the basis for reading and writing skills. The former nurse, who later earned two doctorates, focuses on what she calls the aha! instant—an abrupt transition in electrical activity in the brain that signals that something new has been recognized [see “The Aha! Moment,” by Nessa Bryce].Researchers at Benasich's lab in Newark, N.J., expose Lucas and other infants to tones of a certain frequency and duration. They then record a change in the electrical signals generated in the brain when a different frequency is played. Typically the electroencephalogram (EEG) produces a strong oscillation in response to the change—indicating that the brain essentially says, “Yes, something has changed”; a delay in the response time to the different tones means that the brain has not detected the new sound quickly enough.
The research has found that this pattern of sluggish electrical activity at six months can predict language issues at three to five years of age. Differences in activity that persist during the toddler and preschool years can foretell problems in development of the brain circuitry that processes the rapid transitions occurring during perception of the basic units of speech. If children fail to hear or process components of speech—say, a “da” or a “pa”—quickly enough as toddlers, they may lag in “sounding out” written letters or syllables in their head, which could later impede fluency in reading. These findings offer more rigorous confirmation of other research by Benasich showing that children who encounter early problems in processing these sounds test poorly on psychological tests of language eight or nine years later.
If Benasich and others can diagnose future language problems in infants, they may be able to correct them by exploiting the inherent plasticity of the developing brain—its capacity to change in response to new experiences. They may even be able to improve basic functioning for an infant whose brain is developing normally. “The easiest time to make sure that the brain is getting set up in a way that's optimal for learning may be in the first part of the first year,” she says.
Games, even in the crib, could be one answer. Benasich and her team have devised a game toy that trains a baby to react to a change in tone by turning the head or shifting the eyes (detected with a tracking sensor). When the movement occurs, a video snippet plays, a reward for good effort.
In a study reported in 2014 babies who went through this training detected tiny modulations within the sounds faster and more accurately than did children who only listened passively or had no exposure to the sounds at all. Based on this research, Benasich believes that the game would assist infants impaired in processing these sounds to respond more quickly. She is now working on an interactive game that could train infants to perceive rapid sound sequences.
The Number Sense
Flexing cognitive muscles early on may also help infants tune rudimentary math skills. Stanislas Dehaene, a neuroscientist at the French National Institute of Health and Medical Research, is a leader in the field of numerical cognition who has tried to develop ways to help children with early math difficulties. Babies have some capability of recognizing numbers from birth. When the skill is not in place from the beginning, Dehaene says, a child may later have difficulty with arithmetic and higher math. Interventions that build this “number sense,” as Dehaene calls it, may help the slow learner avoid years of difficulty in math class.This line of research contradicts that of famed psychologist Jean Piaget, who contended that the brains of infants are blank slates, or tabula rasa, when it comes to making calculations in the crib. Children, in Piaget's view, have to develop a basic idea of what a number is from years of interacting with blocks, Cheerios or other objects. They eventually learn that when the little oat rings get pushed around a table, the location differs, but the number stays the same.
The neuroscience community has amassed a body of research showing that humans and other animals have a basic numerical sense. Babies, of course, do not spring from the womb performing differential equations in their head. But experiments have found that toddlers will routinely reach for the row of M&Ms that has the most candies. And other research has demonstrated that even infants only a few months old comprehend relative size. If they see five objects being hidden behind a screen and then another five added to the first set, they convey surprise if they see only five when the screen is removed.
Babies also seem to be born with other innate mathematical abilities. Besides being champion estimators, they can also distinguish exact numbers—but only up to the number three or four. Dehaene was instrumental in pinpointing a brain region—a part of the parietal lobe (the intraparietal sulcus)—where numbers and approximate quantities are represented. (Put a hand on the rear portion of the top of your head to locate the parietal lobe.)
The ability to estimate group size, which also exists in dolphins, rats, pigeons, lions and monkeys, is probably an evolutionary hand-me-down that is required to gauge whether your clan should fight or flee in the face of an enemy and to ascertain which tree bears the most fruit for picking. Dehaene, along with linguist Pierre Pica of the National Center for Scientific Research in France and colleagues, discovered more evidence for this instinctive ability through work with the Mundurukú Indians in the Brazilian Amazon, a tribe that has only an elementary lexicon for numbers. Its adult members can tell whether one array of dots is bigger than another, performing the task almost as well as a French control group did, yet most are unable to answer how many objects remain when four objects are removed from a group of six.
This approximation system is a cornerstone on which more sophisticated mathematics is constructed. Any deficit in these innate capacities can spell trouble later. In the early 1990s Dehaene hypothesized that children build on their internal ballpark estimation system for more sophisticated computations as they get older. Indeed, in the years since then, a number of studies have found that impaired functioning of the primitive numerical estimation system in youngsters can predict that a child will perform poorly in arithmetic and standard math achievement tests from the elementary years onward. “We realize now that the learning of a domain such as arithmetic has to be founded on certain core knowledge that is available already in infancy,” Dehaene says.
It turns out that dyscalculia (the computational equivalent of dyslexia), which is marked by a lag in computational skills, affects 3 to 7 percent of children. Dyscalculia has received much less attention from educators than dyslexia has for reading—yet it may be just as crippling. “They earn less, spend less, are more likely to be sick, are more likely to be in trouble with the law, and need more help in school,” notes a review article that appeared in Science in May 2011.
As with language, early intervention may help. Dehaene and his team devised a simple computer game they hope will enhance mathematical ability. Called the Number Race, it exercises these basic abilities in children aged four to eight. In one version, players must choose the larger of two quantities of gold pieces before a computer-controlled opponent steals the biggest pile. The game adapts automatically to the skill of the player, and at the higher levels the child must add or subtract gold before making a comparison to determine the biggest pile. If the child wins, she advances forward a number of steps equal to the gold just won. The first player to get to the last step on the virtual playing board wins.
The open-source software, which has been translated into eight languages, makes no hyperbolic claims about the benefits of brain training. Even so, more than 20,000 teachers have downloaded the software from a government-supported research institute in Finland. Today it is being tested in several controlled studies to see whether it prevents dyscalculia and whether it helps healthy children bolster their basic number sense.
Get Ahold of Yourself
The cognitive foundations of good learning depend heavily on what psychologists call executive function, a term encompassing such cognitive attributes as the ability to be attentive, hold what you have just seen or heard in the mental scratch pad of working memory, and delay gratification. These capabilities may predict success in school and even in the working world. In 1972 a famous experiment at Stanford University—“Here's a marshmallow, and I'll give you another if you don't eat this one until I return”—showed the importance of executive function. Children who could wait, no matter how much they wanted the treat, did better in school and later in life.
In the 21st century experts have warmed to the idea of executive function as a teachable skill. An educational curriculum called Tools of the Mind has had success in some low-income school districts, where children typically do not fare as well academically compared with high-income districts. The program trains children to resist temptations and distractions and to practice tasks designed to enhance working memory and flexible thinking.
In one example of a self-regulation task, a child might tell himself aloud what to do. These techniques are potentially so powerful that in centers of higher learning, economists now contemplate public policy measures to improve self-control as a way to “enhance the physical and financial health of the population and reduce the rate of crime,” remark the authors of a study that appeared in 2011 in the Proceedings of the National Academy of Sciences USA.
Findings from neuroscience labs have bolstered that view and have revealed that the tedium of practice to resist metaphorical marshmallows may not be necessary. Music training can work as well. Echoing the Battle Hymn of the Tiger Mother, researchers are finding that assiduous practice of musical instruments may yield a payoff in the classroom—invoking shades of “tiger mom” author Amy Chua, who insisted that her daughters spend endless hours on the violin and piano. Playing an instrument may improve attention, working memory and self-control.
Some of the research providing such findings comes from a group of neuroscientists led by Nina Kraus of Northwestern University. Kraus, head of the Auditory Neuroscience Laboratory there, grew up with a diverse soundscape at home. Her mother, a classical musician, spoke to the future neuroscientist in her native Italian, and Kraus still plays the piano, guitar and drums. “I love it—it's a big part of my life,” she says, although she considers herself “just a hack musician.”
Kraus has used EEG recordings to measure how the nervous system encodes pitch, timing and timbre of musical compositions—and whether neural changes that result from practicing music improve cognitive faculties. Her lab has found that music training enhances working memory and, perhaps most important, makes students better listeners, allowing them to extract speech from the all-talking-at-once atmosphere that sometimes prevails in the classroom.
Musical training as brain tonic is still in its infancy, and a number of questions remain unanswered about exactly what type of practice enhances executive function: Does it matter whether you play the piano or guitar or whether the music was written by Mozart or the Beatles? Critically, will music classes help students who have learning difficulties or who come from low-income school districts?
But Kraus points to anecdotal evidence suggesting that music training's impact extends even to academic classes. The Harmony Project provides music education to low-income youngsters in Los Angeles. Dozens of students participating in the project have graduated from high school and gone on to college, usually the first in their family to do so.
Kraus has worked with the Harmony Project and published a study in 2014 that showed that children in one of its programs who practiced a musical instrument for two years could process sounds closely linked to reading and language skills better than children who only did so for a year. Kraus is an advocate of the guitar over brain games. “If students have to choose how to spend their time between a computer game that supposedly boosts memory or a musical instrument, there's no question, in my mind, which one is more beneficial for the nervous system,” Kraus says. “If you're trying to copy a guitar lead, you have to keep it in your head and try to reproduce it over and over.”
Hype Alert
As research continues on the brain mechanisms underlying success in the “four Rs,” three traditional ones with regulation of one's impulses as the fourth, many scientists involved with neuroeducation are taking pains to avoid overhyping the interventions they are testing. They are eager to translate their findings into practical assistance for children, but they are also well aware that the research still has a long way to go. They know, too, that teachers and parents are already bombarded by a confusing raft of untested products for enhancing learning and that some highly touted tools have proved disappointing.
In one case in point, a small industry developed several years ago around the idea that just listening to a Mozart sonata could make a baby smarter, a contention that failed to withstand additional scrutiny. Kraus's research suggests that to gain any benefit, you have to actually play an instrument, exercising auditory-processing areas of the brain: the more you practice, the more your abilities to distinguish subtleties in sound develop. Listening alone is not sufficient.
Similarly, even some of the brain-training techniques that claim to have solid scientific proof of their effectiveness have been questioned. A meta-analysis that appeared in the March 2011 issue of the Journal of Child Psychology and Psychiatryreviewed studies of perhaps the best known of all brain-training methods—software called Fast ForWord, developed by Paula A. Tallal of Rutgers, Michael Merzenich of the University of California, San Francisco, and their colleagues. The analysis found no evidence of effectiveness in helping children with language or reading difficulties. As with the methods used by Benasich, a former postdoctoral fellow with Tallal, the software attempts to improve deficits in the processing of sound that can lead to learning problems. The meta-analysis provoked a sharp rebuttal from Scientific Learning, the maker of the software, which claimed that the selection criteria were too restrictive, that most studies in the analysis were poorly implemented and that the software has been improved since the studies were conducted.
The clichéd refrain—more research is needed—applies broadly to many endeavors in neuroeducation. Dehaene's number game still needs fine adjustments before it receives wide acceptance. One controlled study showed that the game helped children compare numbers, although that achievement did not carry over into better counting or arithmetic skills. A new version is being released that the researchers hope will address these problems. Yet another finding has questioned whether music training improves executive function and thereby enhances intelligence.
In a nascent field, one study often contradicts another, only to be followed by a third that disputes the first two. This zigzag trajectory underlies all of science and at times leads to claims that overreach. In neuroeducation, teachers and parents have sometimes become the victims of advertising for “science-based” software and educational programs. “It's confusing. It's bewildering,” says Deborah Rebhuhn, a math teacher at the Center School, a special-education institution in Highland Park, N.J., that accepts students from public schools statewide. “I don't know which thing to try. And there's not enough evidence to go to the head of the school and say that something works.”
A Preschool Tune-up
Scientists who spend their days mulling over EEG wave forms and complex digital patterns in magnetic resonance imaging realize that they cannot yet offer definitive neuroscience-based prescriptions for improving learning. The work, however, is leading to a vision of what is possible, perhaps for Generation Z or its progeny. Consider the viewpoint of John D. E. Gabrieli, a professor of neuroscience participating in a collaborative program between Harvard University and the Massachusetts Institute of Technology. In a review article in Science in 2009, Gabrieli conjectured that eventually brain-based evaluation methods, combined with traditional testing, family history and perhaps genetic tests, could detect reading problems by age six and allow for intensive early intervention that might eliminate many dyslexia cases among school-aged children.
One study has already found that EEGs in kindergartners predict reading ability in fifth graders better than standard psychological measures. By undergoing brain monitoring combined with standard methods, each child might be evaluated before entering school and, if warranted, be given remedial training based on the findings that are trickling in today from neuroscience labs. If Gabrieli's vision comes to pass, brain science may imbue the notion of individualized education with a whole new meaning—one that involves enhancing the ability to learn even before a child steps foot in the classroom.
Read the original article Here
- Comments (0)
 Subscribe to our Feed via RSS
Subscribe to our Feed via RSS